9873210 wrote:Even if it's not needed spending tens of millions on a dress rehearsal for Omega (or MERS-2, ... ) is far from the worst use of government money we will see this week.
The great thing about this new generation of vaccines is that actually creating a new one is trivial - it's not much more than typing different letters into a computer. Working out which letters to type into the computer is a bit more difficult, but potentially not much more than a few days work. And whilst manufactuing is inherently the same, there would be some minor issues on the logistics side having two SKUs rather than one. The bottleneck is trials and approval. With flu there's a fairly well-established process that once the basic principle of a vaccine is established, the annual variants get an accelerated trial process. We've not done that before with this new generation of vaccines, but AIUI a framework has been established in principle.
So it's been a fairly trivial process to make new vaccines against new variants, and to answer the above thread - there have been trials with Alpha, Beta, Delta & Alpha/Delta-mix vaccines. The real issue is whether you want to use them if the "classic" vaccine is good enough. The classic vaccines are the best understood as they have been given to billions of people, and logistically it's a lot easier if you just have one kind of vaccine to worry about inventory management for, which is important if you're trying to vax as rapidly as possible. Also T cell epitopes seem to be pretty highly conserved in this virus so far. So you need a good reason to not use the classic jab.
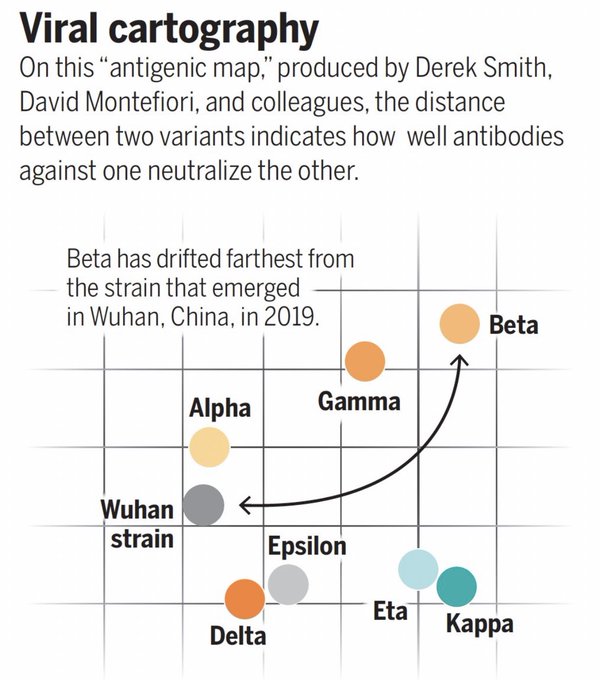
Which is where the concept of mapping antigen space comes in. For the last 18 months the virus has been pushing against the boundaries of antigenic space but not getting very far from the original virus, which is why the original jabs still work well. Omicron is the first variant that sounds like it might have escaped a bit from that original space, but the experts are still debating whether it's worth rolling out a new omicron vaccine.
One reason for that is that SARS2, like flu, shows signs of "original antigenic sin" or immune imprinting, where your immune response is forever shaped by the variant that you are first exposed to. So for instance, an Imperial/QMUL study found that people who got alpha ("Kent") first had stronger responses to delta and weaker responses to beta than people whose first exposure was to the original Wuhan variant.
So...it's complicated, and it's too soon to say for sure.
Antigen mapping pre-omicron :
https://www.science.org/content/article ... us-do-next
Layman's version of the imprinting study :
https://www.imperial.ac.uk/news/232396/ ... rotection/